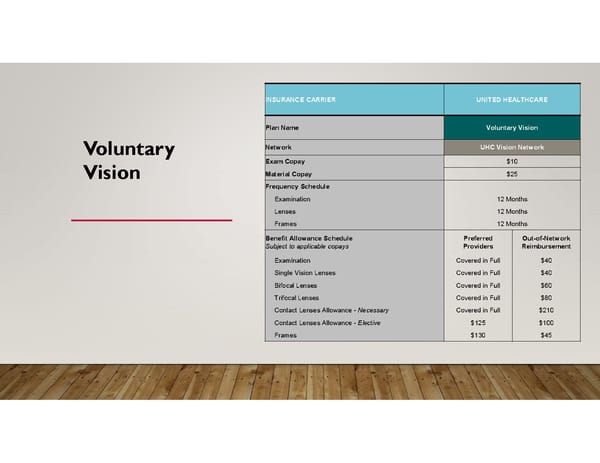
INSURANCE CARRIER UNITED HEALTHCARE Plan Name Voluntary Vision Network UHC Vision Network Voluntary Exam Copay $10 Material Copay $25 Vision Frequency Schedule Examination 12 Months Lenses 12 Months Frames 12 Months Benefit Allowance Schedule Preferred Out-of-Network Subject to applicable copays Providers Reimbursement Examination Covered in Full $40 Single Vision Lenses Covered in Full $40 Bifocal Lenses Covered in Full $60 Trifocal Lenses Covered in Full $80 Contact Lenses Allowance - Necessary Covered in Full $210 Contact Lenses Allowance - Elective $125 $100 Frames $130 $45
 inKind Open Enrollment Page 7 Page 9
inKind Open Enrollment Page 7 Page 9