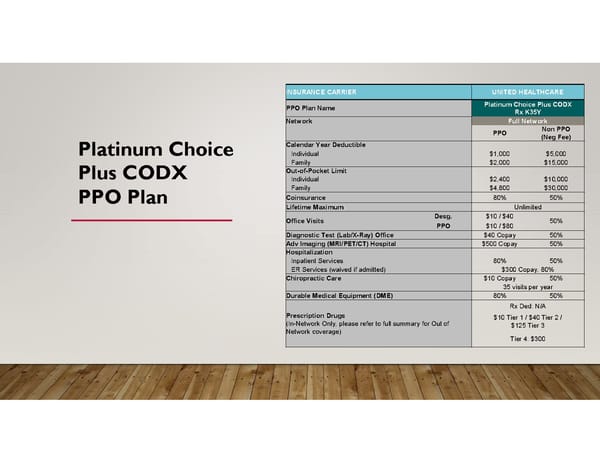
INSURANCE CARRIER UNITED HEALTHCARE Platinum Choice Plus CODX PPO Plan Name Rx K35Y Network Full Network Non PPO PPO (Neg Fee) Calendar Year Deductible Platinum Choice Individual $1,000 $5,000 Family $2,000 $15,000 Out-of-Pocket Limit Plus CODX Individual $2,400 $10,000 Family $4,800 $30,000 Coinsurance 80% 50% PPO Plan Lifetime Maximum Unlimited Desg. $10 / $40 Office Visits 50% PPO $10 / $80 Diagnostic Test (Lab/X-Ray) Office $40 Copay 50% Adv Imaging (MRI/PET/CT) Hospital $500 Copay 50% Hospitalization Inpatient Services 80% 50% ER Services (waived if admitted) $300 Copay, 80% Chiropractic Care $10 Copay 50% 35 visits per year Durable Medical Equipment (DME) 80% 50% Rx Ded: N/A Prescription Drugs $10 Tier 1 / $40 Tier 2 / (In-Network Only; please refer to full summary for Out of $125 Tier 3 Network coverage) Tier 4: $300
 inKind Open Enrollment Page 5 Page 7
inKind Open Enrollment Page 5 Page 7